Emergency Management of Thermal Burns
ABC
Airway & Breathing : Breathing assessed, a patent airway established immediately, airway esbablished and humidified 100% O2 given by mask or nasal cannula or endotracheal tube and initiate manual ventilation - encourage coughing/suctioning/bronchial suctioning. if needed use ventilator, monitor arteerial blood gas values, pulse oximetry readings, carboxyyhemoglobin levels, look for hypoxia
Circulatory system assessed : apical pulse and blood pressure monitored freuently- remove blood pressure cuff after each reading - pulse rate less than 110/minute aimed at.
Insert a large bore IV line Prevent shock by IV fluids(Ringer's solution, normal saline, colloids, whole blood, plasma and plasma expanders used.
Serum electrolytes to be measured. Monitor vital signs. Look for dehydration or overload of fluids.
Consensus formula :
2 to 4 mL/kg/% TBSA (Total Burnt Surface Area)
for a 70 kg man with 50% burns
2 × 70 × 50 = 7,000 mL/24 hours
Plan to administer: First 8 hours = 3,500 mL, or 437 mL/
hour; next 16 hours = 3,500 mL, or 219 mL/hour
Guard against compartmental syndrome : Doppler study the circulation in the limbs. Exchorotomy when needd.
Monitor urinary ouput; watch out for acute renal failure - BUN, serum creatinine, look for hemoglobin or myoglobin - 30-50 ml/hour ideal
Head to toe survey to identify potentially life threatening injuries - cervical spinal injuries, head injuries - treatment initiated
Respiratory System
Look for erythema or blistering oflips or buccdal mucosa, singed nostrils, burns of face, neck or chest, increasing hoarseness, soot in sputum or tracheal tissue in respiratory secretions - chest X-Ray
Wound management
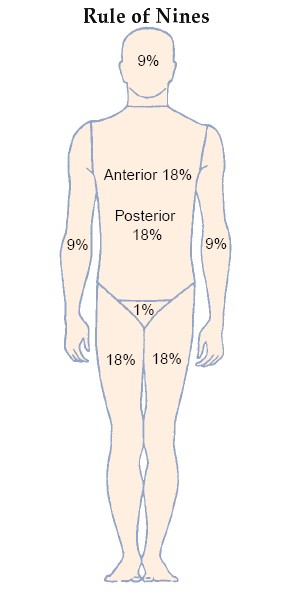
Wound assessment according to rule of nines
Attending to the wound
Frequent short moments of wrapping the wounds with ordinary cool water-soaked towels (not cold or ice cool water)
Remove clothes except the very adherent
Cover the wound with sterile dressings to prevent infection.
Prevention of infection
Take all aseptic precautions from the very beginning
Common bacteria infecting the burn wound : Staphylococcs, Proteus, Pseudomonas, Excherichia coli, and Klebsiella
Fungi and Candida albicans also grow easily in burn wounds
Topical antibacterial therapy started - Silver sulfadiazine, silver nitrate 0.5 % aqueous solution
Pain relief - opioid analgesics, antianxiety medication if needed
Prevention or treatment of complications including carbon monoxide poisoning and infection
Nutritional support; assess the bowel sounds, look for paralytic ileus and abdominal distention; look for occult blood in stools → curling's ulcer and upper GI bleeding → Pantaprazole needed
H/O pre-existing diseases elicited
Assess for progressive edema as fluid shifts occur; elevate affected limbs

.jpg)